

by Steve Kirsch, Steve Kirsch’s newsletter:
 The California Department of Public Health supplied a nonsensical answer when asked to explain the rise in the California COVID case fatality rate (CFR) after the COVID shots rolled out.
The California Department of Public Health supplied a nonsensical answer when asked to explain the rise in the California COVID case fatality rate (CFR) after the COVID shots rolled out.
Executive summary
- Under oath
- If a public official they report to asks them
I chose method #2.
TRUTH LIVES on at https://sgtreport.tv/
Supervisor Sue Frost (Sacramento), the only red pilled Board of Supervisors member in the US (as far as I know), asked the question of her county health officer as to why the CFR went the wrong way after the shots rolled out (it went up instead of down).
The county health officer didn’t know so she had the California Department of Public Health (CDPH) respond directly.
Their answer was nonsensical.
So now you know too.
The question Supervisor Frost posed to the Health official in Sacramento
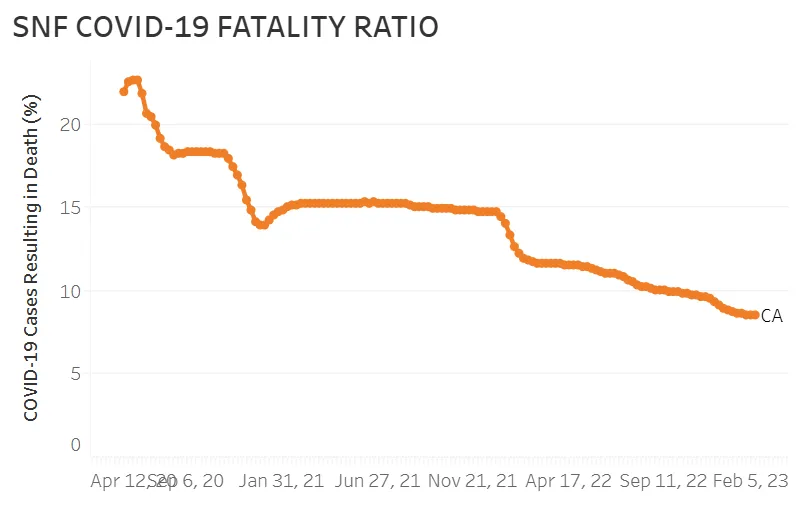
The Fatality Ratio graph from the CDPH that you provided in your previous response shows that the Fatality Ratio reversed direction (went up) instantly after the COVID shots were introduced, and then remained flat for nearly a year until Omicron. If the COVID vaccine worked, wouldn’t you have expected the Fatality Ratio to go down over time as more people were vaccinated rather than remain flat? The variant didn’t change until later in 2021! And why would it go up right after vaccination? Was it predicted it would go up and then remain flat?
The CDPH answer
COVID-19 vaccines first became available in the middle of a surge in COVID-19 disease in late 2020 and early 2021. The risk of death increased during the surge for those who were not yet vaccinated. Meanwhile, it took several months after COVID-19 vaccines first became available for many long-term care residents to be vaccinated against COVID-19.
The Fatality Ratio of residents in facilities included a mixture of unimmunized individuals and immunized individuals. Comparing the mortality between unvaccinated versus vaccinated residents would better indicate the protective effect of vaccination.
More rigorous evidence of the effectiveness of COVID-19 vaccine in protecting residents of long-term care facilities against severe COVID-19 infection and death includes, but is not limited to, the studies linked at:
- Real-world Effectiveness of mRNA COVID-19 Vaccines Among US Nursing Home Residents Aged ≥65 Years in the Pre-Delta and High Delta Periods | Open Forum Infectious Diseases
- BNT162b2 mRNA COVID-19 (Comirnaty) Vaccine Effectiveness in Elderly Patients Who Live in Long-Term Care Facilities: A Nationwide Cohort | Gerontology
- Association of BNT162b2 Vaccine Third Dose Receipt with Incidence of SARS-CoV-2 Infection, COVID-19–Related Hospitalization, and Death Among Residents of Long-term Care Facilities, August to October 2021 | Infectious Diseases | JAMA Network Open | JAMA Network
- Association of Receipt of the Fourth BNT162b2 Dose with Omicron Infection and COVID-19 Hospitalizations Among Residents of Long-term Care Facilities | JAMA Internal Medicine
- Effectiveness of a fourth dose of covid-19 mRNA vaccine against the omicron variant among long term care residents in Ontario, Canada: test negative design study | The BMJ
- Effectiveness of a fourth dose of mRNA COVID-19 vaccine against all-cause mortality in long-term care facility residents and in the oldest old: A nationwide, retrospective cohort study in Sweden | The Lancet Regional Health Europe
My analysis
If you have a FIXED known group of people and you give 98% a vaccine that is supposed to reduce their COVID mortality by 50%, the mortality should go down.
It doesn’t get any more complicated than that.
No fancy math required. No Cox regression analysis needed. All raw data.
If the vaccine works, the numbers have to go down.
Read More @ kirschsubstack.com