

by Brian Shilhavy, Health Impact News:
The Flu did not disappear, it was simply rebranded as Covid. With further commentary from the longtime lead scientist of the CDC’s molecular diagnostic laboratory.
by Jordan Schachtel
The Dossier
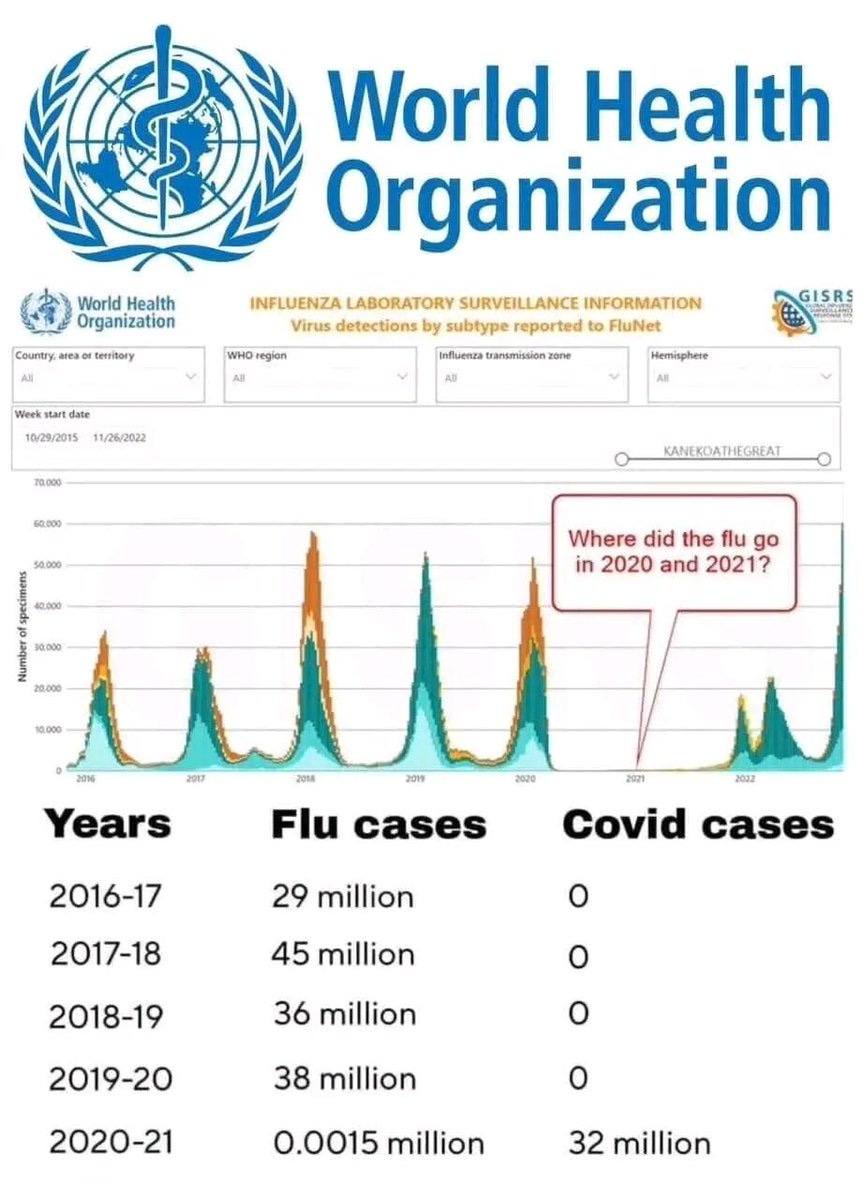
One of the biggest mysteries of “the pandemic” involves the supposed disappearance of the flu. Did the flu really disappear during the covid hysteria era, or is something else afoot?
TRUTH LIVES on at https://sgtreport.tv/
Now, during the confusion and panic of the last few years, there have been lots of explanations advanced about the supposed disappearance of the flu. The lockdowners and their credentialed institutions often claimed that masked worked (lol) to stop the flu, despite not working for covid. Others claimed that covid had some kind of viral dominance effect that defeated influenza strains.
But neither explanation really solves the “where did the flu go” mystery.
The evidence seems to point to two main reasons for the flu’s disappearance: the physical disappearance of flu testing kits and a misunderstanding of what the flu actually means.
- The flu tests were not physically available in healthcare systems
The Dossier surveyed several individuals and organizations with access to hospital system records and supply chain management, and we pooled together lots of anecdotal information to paint a greater picture of what happened.
We found that, at least in the United States, there was virtually no access to flu testing during the covid hysteria years, particularly from 2020 to 2021. Virtually all testing manufacturers pivoted to covid testing, leaving the influenza kits behind. According to Pharma and Government Health, Covid was a much bigger priority, both from a healthcare perspective and a business perspective, so the flu industry was no longer lucrative and kicked to the curb.
The second reason, however, is even more important.
- The flu is not understood in its proper context
Prior to the establishment of the covid testing industrial complex (which brought in well over $100 billion a year at its peak), flu was almost always diagnosed by symptoms, not by a swab test. And again, covid symptoms are virtually identical to flu symptoms.
In the vast majority of cases, what is “the flu” is traditionally understood not as a viral influenza diagnosis but a general diagnosis of countless potential symptoms categorized in a broad category as “flu.”
Very few doctor-diagnosed “flu” cases actually come from influenza strains. This is why it is the perfect rationale to understand covid as the flu but with scarier branding. Both flu and covid share the same symptoms, so a potential flu case/illness/death instead was generally diagnosed as a covid case/illness/death.
But enough from your humble correspondent. Let’s read a more detailed response from someone who knows this issue very well.
I also posed this question to Dr Norman Pieniazek (follow him on Twitter), a renowned molecular biologist who worked at the Centers for Disease Control (CDC) as the head of its molecular diagnostic laboratory for 24 years. Dr Pieniazek is an expert in PCR testing diagnostics and has a fascinating perspective on the shoddy science behind “the pandemic.”
Here’s his reply to my question:
From Dr. Norman J. Pieniazek:
Did the flu disappear during the COVID-19 pandemic?
I will try to answer this question; however, first, I must explain the terms common cold and flu (influenza).
Do you know that over 200 viruses cause colds and that people in the United States suffer from an estimated 1 billion colds yearly (1)? Nonetheless, can we clearly say who suffers from the common cold and the flu? What about PCR, the technique used to monitor the cases of COVID-19? Unfortunately, PCR was found to be impractical for the diagnosis of infections of the respiratory tract for at least two reasons.
The first problem is the diagnostic sample. Mucus samples, taken from deep nostrils (nasal swab), throat (oropharyngeal swab), and nasopharynx (nasopharyngeal swab), in essence, test the human air filter. The nasal passages have ridges that cause the air to swirl, similar to the Dyson vacuum cleaner principle. As the nasal passages and the whole respiratory tract are lined with mucus, it traps viruses, bacteria, pollen, fungal spores, and dust. This layer with trapped particles is moved by ciliated cells out of the airways (2). When the mucus is tested with PCR, detecting a part of a virus in the air filter doesn’t mean that this virus caused the infection. This problem with swabs has been known for a long time (3). The consensus is that broncho-alveolar lavage (BAL) is the most appropriate specimen for detecting respiratory tract viral infections. Unfortunately, collecting the BAL sample is complex and may not be approved by the patient (4).
The second problem was signaled above. With more than 200 possible infection causes (etiology), testing for all suspects is not feasible. While in a scientific study (3, 5), no stone would be left unturned to diagnose patients enrolled in a project, surveillance cannot be done this way.
CDC has developed a sentinel system for monitoring colds in the US population. This system monitors visits for respiratory illnesses, including fever, cough, or sore throat. Such visits are classified as Influenza-Like Illnesses (ILI). Please note that this designation doesn’t imply laboratory-confirmed influenza and captures patient visits due to all respiratory pathogens that cause similar symptoms (6). In addition to this system, CDC collects data on confirmed influenza cases (7); however, only about 1% of samples tested are usually positive. The take-home message is that no one knows how many flu cases are in the US annually. The reported number of ILI may be only the tip of the iceberg.
With the arrival of the Wuhan virus in January 2020, all lessons of prior seasons were forgotten. People were forced to be tested even when they showed no symptoms. Despite ample evidence to the contrary, PCR done from swabs was suddenly advertised as the gold standard for diagnosis of infections of the respiratory system. Consider another important fact. In a carefully conducted study (4) of hospitalized pneumonia patients diagnosed on classical X-Ray or CAT scans, the cause of the infection (etiology) could not be established in 62% of cases. How is it possible that during the pandemic in the US, there were 107,201,630 COVID infections and 1,166,899 COVID deaths as of today (8)? Where are infections with other viruses? Where are conditions of unknown etiology?
Read More @ HealthImpactNews.com